Extreme Picky Eating or Eosinophilic Oesophagitis?

Embarking on the journey of understanding extreme picky eating in children, it is crucial to acknowledge the complexity often hidden beneath seemingly typical behaviours. It is easy to dismiss picky eating as a mere behavioural issue or attribute it solely to sensory challenges. Among some practitioners, the go-to explanation might be deficiencies in zinc or iron. While these factors are indeed potential contributors and should be considered, it is essential to recognise that, in many cases, the root of the problem runs much deeper.
Today, we delve into the realm of Eosinophilic Oesophagitis (EoO), a condition that can underpin issues of Avoidant Restrictive Food Intake Disorder (ARFID) and extreme pickiness. Eosinophilic Oesophagitis presents a unique challenge in children with autism, PANDAS, and PANS, requiring a holistic approach that goes beyond mainstream treatments. Functional medicine offers individualised strategies focusing on identifying root causes and supporting overall health.
Understanding Eosinophilic Oesophagitis (EoO):
Eosinophilic Oesophagitis is a complex interplay of food allergies and swallowing disorders, identified as a chronic immune system condition. It is characterised by the presence of eosinophils, a kind of white blood cell typically found in the digestive tract, that accumulates in the oesophagus, leading to chronic swelling and potential complications such as scarring and strictures. The trigger could be a response to a food allergen, environmental allergens like pollen, or long-term gastric acid reflux. About 50% of individuals with EoO also have seasonal allergies or asthma.
Early life exposure plays a pivotal role in influencing the risk of developing EoO. Various factors during infancy can significantly impact susceptibility to EoO later in life. Research has shown that exposure to antibiotics in infancy increases the risk of EoO six-fold, underscoring the potential long-term consequences of early antibiotic use. Similarly, infants born via Caesarean section face a 2.2-fold increased risk, while preterm birth is associated with a 4.2-fold elevated risk. Non-exclusive breastfeeding, maternal smoking, and Group B Streptococcus (GBS) exposure also contribute to heightened risks, with non-exclusive breastfeeding linked to a 3.5-fold increase, maternal smoking doubling the risk, and GBS exposure resulting in a 2.2-fold higher likelihood of developing EoO.
Several additional factors may also contribute to a heightened risk of developing EoO. Variations in the microbial communities within the body, known as the microbiome, can play a key role in increasing susceptibility to EoO. Furthermore, seasonality has been identified as a factor, with a notable increase in cases during the spring and summer months. Climate also plays a role, with EoO being more common in temperate climates compared to tropical regions. Additionally, the geographical location appears to influence the prevalence, with higher incidences noted in urban and rural areas. Interestingly, very few cases are reported in tropical areas and developing countries, indicating potential environmental and geographical correlations with the occurrence of EoO. Understanding these diverse factors is essential for a comprehensive approach to addressing and managing the risk factors associated with EoO.
Symptoms of EoO:
Symptoms of EoO can manifest differently across various age groups. In infants and toddlers, clinical presentations often involve feeding difficulties, picky eating, and failure to thrive. School-age children may experience symptoms such as nausea, vomiting, pain, heartburn, and reflux. Conversely, adults with EoO may exhibit solid food dysphagia, as if food is stuck in the throat, and may also face issues like food impaction. The hallmark symptom, regardless of age, is difficulty swallowing, often accompanied by sensations of food getting stuck. Additional symptoms may include heartburn, chest pain, coughing, and abdominal pain.
Diagnosing EoO:
Various tests, including upper endoscopy, biopsies, blood tests, and dietary assessments, play a crucial role in confirming EoO in children.
Medications for EoO:
Acid blockers, topical steroids, and, if necessary, systemic steroids like prednisone may comprise part of the treatment plan. Using medications is never ideal, but sometimes it can be necessary, and we can work to wean off over time with the support of the medical team.
Dilation for EoO:
In cases of strictures, dilation procedures may be considered, balancing potential benefits with risks.
In our clinic, we work closely with medical teams and focus on the following functional medicine approach.
Taking Action: Evidence-Based Strategies
Dietary Changes and Modifications:
Identifying and eliminating trigger foods is essential. Recent studies indicate that specific food triggers contribute significantly to EoO symptoms. Dairy emerges as a predominant trigger in 74% of cases, followed by wheat and gluten in 26%, eggs in 17%, soy in 10%, and peanuts in 6%. Other triggers tend to be less prevalent, often associated with fish and seafood. It is important not to rely entirely on assessing allergies by measuring IgE markers but also to include IgG testing to uncover intolerances, which can take up to 72 hours to manifest after ingestion.
Elemental diets or allergen-free formulas may be necessary for severe cases. We often work with children whose medical needs are being managed by a medical team, using the tools available to us to support health and play our role in building health from the ground up. The chart below highlights the comparison of the success rates of the various dietary interventions.
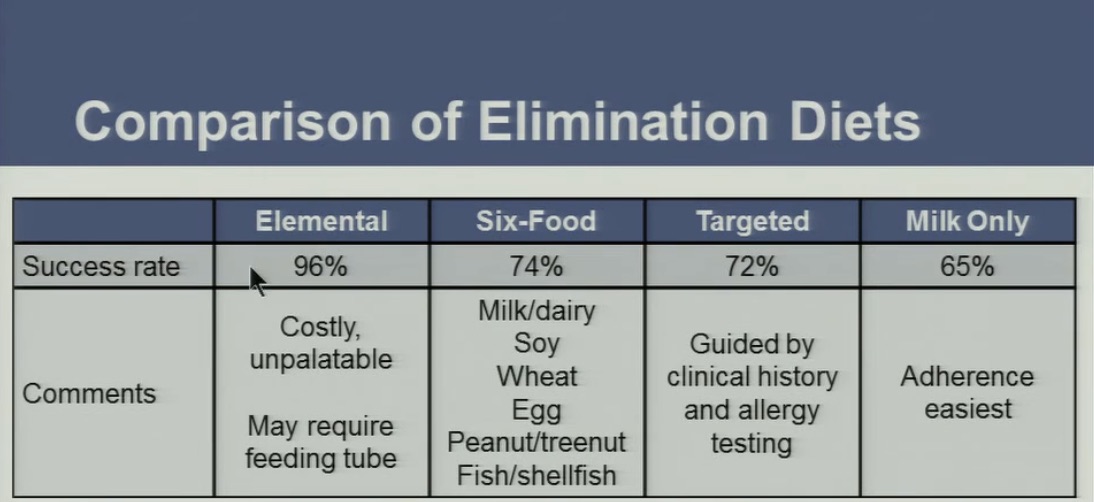
Source: Delton, Gastroenterology, 2014
Identification of Food Allergies and Sensitivities:
In the Functional Medicine approach, a meticulous exploration of the root causes of EoO is crucial. Employing specialised food sensitivity panels measuring immunoglobulin IgG levels can unveil potential triggers contributing to eosinophil accumulation in the oesophagus. The subsequent elimination of identified sensitivities from the diet aims to address the core issues fuelling EoO symptoms. We also consider IAG and dietary-derived peptide testing.
Reducing Inflammation:
Inflammation is a key contributor to the difficulty swallowing experienced with EoO. It is vital to manage inflammation, which can often be reduced by making the appropriate dietary adjustments. At our clinic, we use various natural compounds such as curcumin, Boswellia, Palmitoylethanolamide (PEA), liquorice, and specific Micro-immunotherapy formulations. It’s a vital part of the process to help make the other deeper work we need to do possible. It’s also vital to use soothing substances such as aloe vera, slippery elm, marshmallow (not to be confused with the soft confectionary!) One of the most healing substances we have used is Siberian pine nut oil, which has helped to reduce reflux and aid in healing the oesophageal lining.
Re-educate the Immune System.
In order to get long-term gains, we need to re-educate the immune system to respond correctly. As part of this process, we rely extensively on Micro-immunotherapy, which has been a game-changer in modulating the immune response.
Support Gut Health:
Maintaining optimal gut health is a pivotal component in managing EoO. A balanced gut microbiota is essential for metabolic harmony, and identifying and rectifying imbalances are fundamental aspects of EoO management. Microbial and yeast overgrowth, as well as potential parasitic infections, can contribute to inflammation, underscoring the need for targeted interventions to restore gut health. The intricate gut-brain connection emphasises how supporting gut health positively influences overall well-being, impacting immune responses crucial for EoO management.
The Brainstorm Health “GUT RESTORE” program provides a comprehensive strategy beyond conventional EoO management approaches. Central to this program is the thorough assessment of gut health through testing, aiming to restore microbial balance and eliminate the overgrowth of yeast, parasites, and pathogenic bacteria. By addressing intolerances, allergies, and triggers like dairy and gluten, the program not only aims for symptom resolution but also recognises the pivotal role of gut health in the holistic and effective management of EoO.
In conclusion, unravelling the complexities of extreme picky eating in children necessitates a comprehensive understanding of conditions like Eosinophilic Oesophagitis. A multi-faceted approach, combining dietary adjustments, medication, and functional medicine strategies, offers hope for managing and alleviating symptoms and fostering a healthier and more vibrant life for affected children.
References:
- Aceves SS. (2011). Eosinophilic esophagitis: an allergic disease? Gastroenterol Clin North Am. 40(1):75-91.
- Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras CA, Katzka DA. (2018). ACG clinical guideline: evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 113(7): 984–1013.
- Dehlink E, Fiebiger E. (2016). The role of the high-affinity IgE receptor, FcεRI, in eosinophilic gastrointestinal diseases. Immunol Allergy Clin North Am. 36(3):611-624.
- Dohil R, Newbury R, Fox L, Bastian J, Aceves S. (2010). Oral viscous budesonide is effective in children with eosinophilic esophagitis in a randomized, placebo-controlled trial. Gastroenterology. 139(2):418-29.
- Lucendo AJ, Molina-Infante J. (2011). Eosinophilic esophagitis. N Engl J Med. 364(13):1271-1278.
- Markowitz JE, Spergel JM, Ruchelli E, Liacouras CA. (2003). Elemental diet is an effective treatment for eosinophilic esophagitis in children and adolescents. Am J Gastroenterol. 98(4):777-82.
- Mueller S, Neureiter D, Aigner T. (2019). Stool markers for diagnosis of pediatric inflammatory bowel disease. J Clin Med. 8(4): 510.
- Philpott H, Nandurkar S, Royce SG, Thien F, Gibson PR. (2018). Allergy tests do not predict food triggers in adult patients with eosinophilic oesophagitis. A comprehensive prospective study using five modalities. Aliment Pharmacol Ther. 47(3):368-374.
- Sleiman PM, Grant TH, Collins MH, Wang N, Grimmett ZW, Wang S, Fulkerson PC. (2017). Mucosal Eosinophilia: Prevalence and Clinical Associations in a Large Prospective Acid Reflux Cohort. Am J Gastroenterol. 112(6): 970–977.
- Straumann A, Bauer M, Fischer B, Blaser K, Simon HU. (2001). Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J Allergy Clin Immunol. 108(6):954-61.

