Food and Mood

Article written by Stella Chadwick for the Spring 2021 issue of the Autism Eye Magazine
Can certain fruits, vegetables, herbs and spices cause negative behavioural issues for our children?
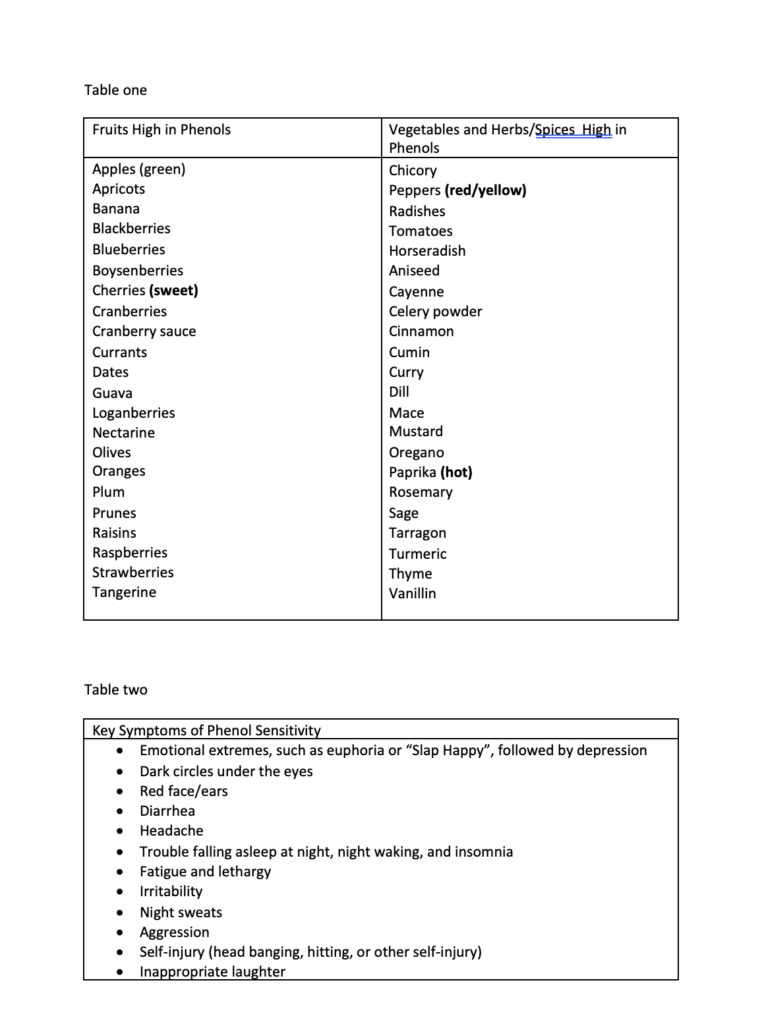
Many of us know, or have figured out through personal experience, that food colouring, additives and flavourings can impact our children’s behaviour and mood. But what is less known is that certain foods that are deemed “super healthy” can also have the same negative effects. This is because of chemical compounds known as polyphenols, found naturally in plant products, which are not able to be processed properly by some children. Some foods, such as berries, cherries, certain types of apples, red grapes, oranges, peppers and tomatoes contain particularly high levels of polyphenols. For a guide to the fruits and vegetables, as well herbs and spices with the highest level of phenols please see table one. Other foods that don’t quite fit into the categories, but can be significantly problematic, for some include cheese and chocolate.
How polyphenols work and impact mood and behaviour
In a healthy body, with a balanced gut microbiome, polyphenols offer many health benefits through their antioxidant activity by protecting our cells from damage from free radicals which can harm our cells and lead to disease. They can also be excellent for our gut microbiome when absorbed and processed correctly. However, in some children these foods are not processed correctly and can build up and overwhelm the body and cause a multitude of symptoms with the key ones outlined in table two. The key chemical that we need to process polyphenols is sulphate, which seems to be in short supply and can be abnormally metabolised in many children with autism.
The most noteworthy research into this topic has been carried out by Rosemary Waring, who is an Honorary Reader in Human Toxicology at University of Birmingham and was the first researcher to produce scientific evidence suggestive of abnormal sulphur metabolism affecting people with autism. In her studies she found that approximately 92% of children with autism had low levels of sulphate in their plasma. When sulphate is in short supply there can be significant impact on neurotransmitters and gut function, leading to food intolerances to many foods. Low sulphate levels mean that the production of an enzyme called PST (Phenol Sulphur Transferase) is diminished. PST deficiency can impair the breakdown of polyphenols, as well certain neurotransmitters such as serotonin and dopamine. It can also impair the uptake of nutrients because of the role it plays in bile and enzyme production. The ultimate effect on the child can be significant impact on mood, behaviour, sleep and ability to focus as well as failure to thrive and generalised gut issues. Those who are sensitive to phenols and/or salicylates often have nervous system over stimulation. There may be immediate indications soon after eating, but there is research to suggest that levels reach their highest point between 1.5 to 5.5 hours after consumption. However, often symptoms can be delayed, sometimes taking up to 72 hours to manifest. For a detailed list of the most common symptoms, we see in our clinics in children who struggle with processing phenols and associated chemicals, please see table two.
Is there a test that can be done?
This is a difficult one as measuring sulphate or enzyme activity can be very tricky and inaccurate. We generally rely on the clinical picture to ascertain the likelihood of a child with this issue. In general, if we work with a child who has lot of food intolerances, as well low level of nutrients such as magnesium, zinc, molybdenum and B6 and responding well to dietary changes and sulphation support (discussed below) then it is likely that poor sulphation may be the root of their many symptoms. It is of note that sulphate is needed to detoxify paracetamol, and if there is extensive use of paracetamol in the medical history of the child exhibiting some of other symptoms of poor sulphation then we can become even more confident about the root cause.
What can we do to improve symptoms?
As an absolute minimum, removing food colouring, additives and preservatives from the diet is a must. In terms of other dietary changes, the key is to reduce the phenolic load by keeping an eye on the foods that have the highest levels and making sure you keep them to a minimum or remove them completely for a few weeks remembering that it is not necessary to remove all sources of phenols but to reduce them significantly in the first few weeks to see if it makes a difference to your child’s symptoms. Lowering phenolic intake is the basis of the Failsafe and the Feingold diets. Through Dr Waring’s research we know that adequate sulphation is required for the integrity of the gut lining and that those children who have low levels of sulphate have been shown to also suffer with compromised gut lining and subsequently from food intolerances. These children are also a lot more likely to be sensitive to gluten and dairy and to amines, for example those found in cheese, chocolate, bananas and citrus fruits. In terms of medication if at all possible, avoid paracetamol-based drugs and speak to your doctor to find alternative solutions. The other strategy is to support the pathway that helps breaks these chemicals down. One of the most powerful tools is the use of Epsom salt baths, taken 3 to 4 times per week, ensuring the use of at least 1 to 2 cups of Epsom salts and allowing the child to soak for at least 20 minutes. If you don’t have a bathtub or your child is averse to it, then use a footbath instead and half the amount of salt you use. If warranted, including supplemental zinc, molybdenum and magnesium and B6 (ensuring the magnesium and B6 are given together as B6 on its own can exacerbate the problem further due to the way it can inhibit the PST enzyme) can also be helpful. Using enzymes that break phenols down can be really effective for some, since it can be almost impossible to avoid phenols completely. We use No-Fenol enzyme by Houston Enzymes. Gut support is crucial for these children, and we use a multitude of techniques to help balance the gut ecosystem and repair the gut.
Conclusion
In clinical practice, I have found that some children can respond within a week or two to lowering phenols and supporting the pathways. Parents report much better mood, better sleep and better focus and concentration. However, where appropriate and indicated, we suggest that families work with a professional and follow through with the diet and targeted nutritional support for at least 6 months. If there are no significant changes then that would be the time to reconsider. Implementing the diet, supporting the sulphation pathways and working on gut health appear to be the key strategies to long term and consistent improvements.
References
Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies Claudine Manach, Gary Williamson, Christine Morand, Augustin Scalbert, Christian Rémésy The American Journal of Clinical Nutrition, Volume 81, Issue 1, January 2005, Pages 230S–242S, https://doi.org/10.1093/ajcn/81.1.230S
Microbial metabolism of dietary phenolic compounds in the colon Anna-Marja Aura Phytochemistry Reviews volume 7, pages407–429(2008) Journal of Nutritional & Environmenta l Medicine (2000) 10, 25–32
Sulphur Metabolism in Autism H. WARING AND L. V. KLOVRZA School of Biosciences, University of Birmingham, Journal of Nutritional & Environmental Medicine (2000) 10, 25–32